Ulcerative Colitis and Crohn's disease
Inflammatory bowel disease refers to a two main diseases, Ulcerative colitis (UC) and Crohn’s disease that cause ulceration and inflammation of the bowel.
Common symptoms include diarrhoea, rectal bleeding, passing mucous, abdominal pain, bloating and sometimes weight loss.
Despite a lot of research the exact cause of these diseases remains unknown. In both cases damage occurs to the bowel due to inflammation that is driven by a dysfunctional and overactive immune system. Treatments are therefore targeted at reducing inflammation and dampening down the immune system.
Crohn’s disease causes inflammation and ulceration of the full thickness of the bowel wall and can involve anywhere in the GI tract including the mouth, stomach, duodenum, jejunum & ileum (small bowel), colon, anus and perianal skin.
Disease sites specific to Crohn's include:
- Ileitis, Ileo-colitis
- Fistuals
- Strictures
Ulcerative colitis (UC) causes inflammation and ulceration of the inner lining of the bowel and effects the colon (large bowel) only.
When UC effects the first part of the rectum we call this "proctitis", when between 10-50cm of bowel is effected "left-sided colitis" and when all of the bowel is effected "pan-colitis".
The extent of the disease dictates which treatments are likely to be most effective.
- Accurate diagnosis of UC and Crohn’s using High-Def endoscopy/colonoscopy, blood tests and biopsy.
- Targeted investigation with MRI, Capsule endoscopy.
- Individualised patient treatment plans.
- Use of Biological Drugs early to prevent complications including:
- Stelara (Ustekinumab)
- Entyvio (Vedolizumab)
- Remicade/Remsima (Infliximab)
- Humira (Adalimumab)
- Xeljanz (Tofacitinib)
- Use of Budesonide to prevent steroid complications when appropriate.
- Access to dose escalation, home infusions and compassionate supplies when needed.
- Attention to disease control and patient quality of life as the highest priority.
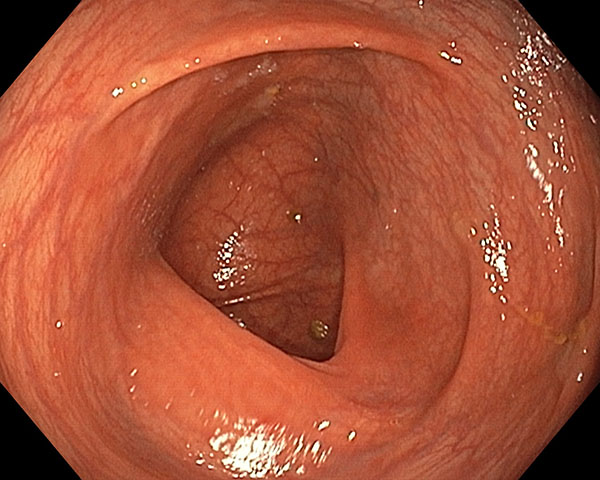
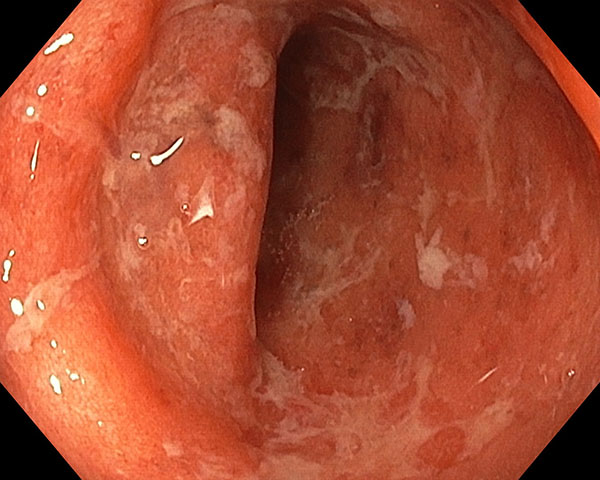
Case 1. UC
23 year old female with presented with up to 10 bloody and mucousy diarrhoea motions per day and abdominal pain. Found to have severe ulcerative colitis of the entire bowel (pan-colitis) on colonoscopy and treated with oral mesalazine 4g (Pentasa) and corticosteroids. To avoid weight gain, budesonide (Cortiment) used instead of prednisone.
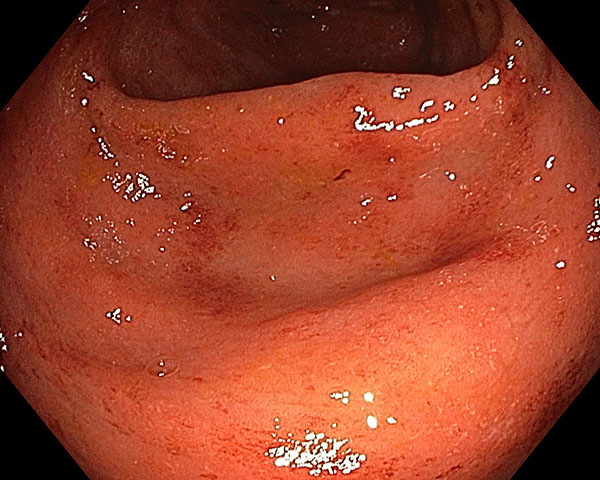
Good response to initial therapy, but frequent flare ups over the following year even after azathioprine (Imuran) trialled for 3 months. Colonoscopy showed extent of disease reduced to 50cm but still active inflammation.
Commenced on vedolizumab (Entyvio) infusions at home and then later transitioned to Entyvio injector-pen given under the skin every 2 weeks. Resolution of all symptoms after just 8 weeks and Colonoscopy 6 months later showed complete remission with healing of all previous changes. Able to cease all other medications and remains in remission.

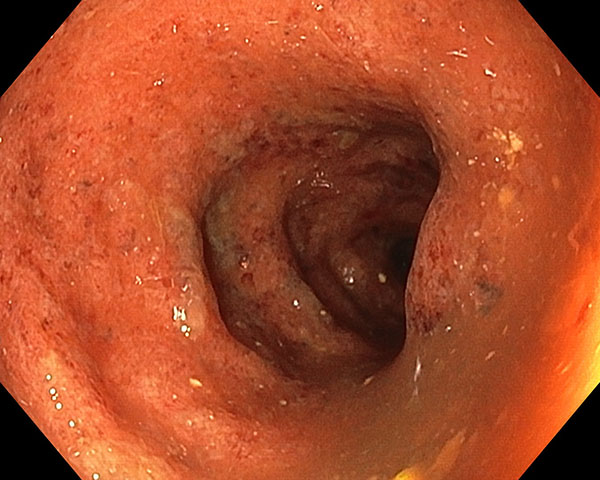
Case 2. Crohn's Disease
34 year old man referred for ongoing management of Crohn's disease with a prior history of ileitis, but currently not on medication. Symptoms of intermittent severe abdominal pain, diarrhoea and occasional mucous leakage.
Found to have ulceration in the right side of the colon, terminal ileum and rectum, in addition to a perianal fistula. MRI enterography showed no other small bowel sites of disease and MRI pelvis showed no abscess associated with the fistula.
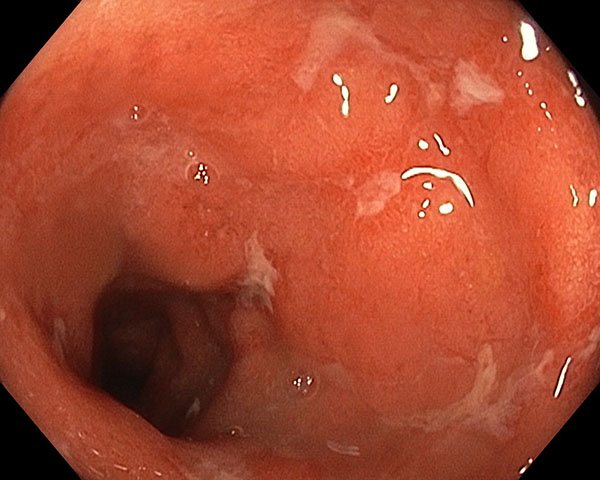
Commenced on the TNF-antagonist Adalimumab (Humira) sub-cut injections every 2 weeks and brief course of corticosteroids. Able to avoid surgery for the fistula with the hole closed over on review 9 months later and close to resolution of ulcers at colonoscopy.
Click on each image to view: